The
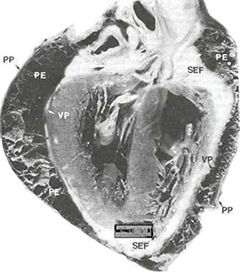
pericardium is a tough, fibrous, outer coating with discrete
attachments to the sternum, great vessels, and diaphragm and
an inner membranous coat.
It is divided into two layers, the first of which is called
the parietal one, and the second the visceral component. The
pericardium contains approximately ten to fifteen cc's of serous
fluid. The function of the pericardium is to limit or prevent
acute pathological distension of the heart once the pericardial
reserve volume has been used up and the pericardium is stretched.
It does not cover the left atrium, which lies anterior to the
pericardium.
The pericardial attachments maintain the heart in its normal
position and are so arranged that external forces exerted on
the pericardium by respiration or changes in body posture tend
to cancel each other and maintain a constant heart position.
(click Play to see video of Swinging of the Heart)
Apical four-chamber two-dimensional echocardiograms show the extremes of oscillation and the resultant effect on the QRS complex. In Panel A, the heart swings to the right, and lead I I shows a small QRS complex. In Panel B, the heart swings to the left, and the QRS complex is larger. P denotes pericardium, and LV left ventricle.
In the recent October 29, 2009 edition of the New England Journal Medicine,October 29,2009 there is a video of a case of a "swinging heart" secondary to a large effusion secondary to stage IV melanoma. Transthoracic echocardiography showed a large pericardial effusion with swinging of the heart (to learn more see video) and collapse of the right atrium (RA) and left atrium (LA) in end diastole (Panel A, arrows) and diastolic collapse of the right ventricle (RV) (Panel B, arrows), which was consistent with pericardial tamponade.
Pericardiocentesis yielded 1.6 liters of bloody fluid; the fluid was subsequently shown to be a malignant effusion. Swinging of the heart that is due to a large pericardial effusion is responsible for the beat-to-beat shift in the axis, amplitude, and morphology of the QRS interval (electrical alternans) on electrocardiography. In this patient, the condition resulted in a "pseudo" 2:1 atrioventricular-block pattern, with an absent QRS interval after every other P wave (Panel A, arrowheads), despite ventricular contraction on echocardiography.
Transthoracic echocardiography showed a large pericardial effusion with swinging of the heart (to learn more see video) and collapse of the right atrium (RA) and left atrium (LA) in end diastole (Panel A, arrows) and diastolic collapse of the right ventricle (RV) (Panel B, arrows), which was consistent with pericardial tamponade. Pericardiocentesis yielded 1.6 liters of bloody fluid; the fluid was subsequently shown to be a malignant effusion. Swinging of the heart that is due to a large pericardial effusion is responsible for the beat-to-beat shift in the axis, amplitude, and morphology of the QRS interval (electrical alternans).
PERICARDIAL
CYSTS
Pericardial, or mesothelial, cysts are the most frequent benign
"tumors" of the pericardium. They are usually found
coincidentally on a routine roentgenogram. However, 25 to 30
percent of the patients will have chest pain, dyspnea, cough,
or paroxysmal tachycardia. Pericardial cysts occur most frequently
in the third or fourth decade of life and equally among men
and women. The right costophrenic location is the most common,
although they may present in the upper mediastinum. Only rarely
does the cyst connect with the pericardial cavity. Clinically
and radiographically, they resemble other tumors of the pericardium.
Hemodynamically significant cardiac-chamber compression rarely
results. Echocardiography. CT scanning, and MRI are most helpful
in the differential diagnosis. Surgical excision completely
relieves symptoms and confirms the diagnosis;however,
percutaneous aspiration of the cystic contents is an attractive
alternative to surgical resection.A case of video-asssisted
surgical excision of a recurrent pericardial cyst has been reported.