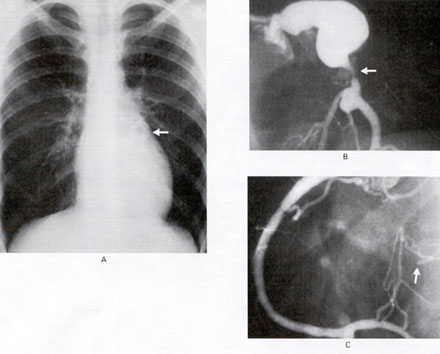
Figure 179
A 14-year-girl in whom Kawasaki's disease was diagnosed at the age of 2years had a posterior myocardial infraction at the age of 3 years. When we saw her she had signs of mild mitral reguritation but no symptons. Transthoracic echocardiography demonstrated a gaint anuerysm involving the left main coronary artery. On exercise testing she had ST-segment depression in leads 1, 11, V4 and V5. Exercise echocardiography confirmed the presence of severe, reversible ischemia of the midportion and distal portion of the anterior wall, apex, distal septum, and lateral wall of the left ventricle. A chest film showed an area of calcification at the upper border of the left ventricle (arrow in Panel A). Selective angiography of the left coronary artery showed a large aneurysm of the left main coronary artery with stenosis of 80% of the luminal diameter at the origin of the left anterior descending artery (arrow in Panel B). The circumflex coronary artery was occluded proximally (not shown) but filled by means of collaterals from the right coronary artery (arrow in Panel C). This patient underwent surgical revascularization because of the poor prognosis associated with the stenosis of a giant anuerysm in a patient with Kawasaki's disease. Three years after surgery, the patient was asymptomatic, and exercise echocardiography demonstrated no inducible ischemia.
Graeme F.Porter,MBm,ChB,Thomas
L. Gentles,FRACP,N ENG J Med,Vol.345,No.2
P.98,July 12,2001.