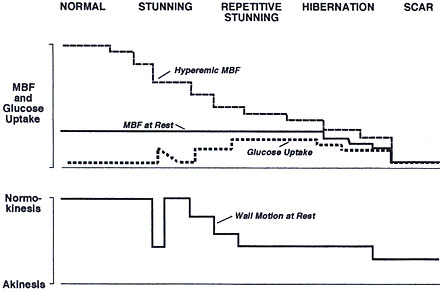
Figure 216-10
Possible time-dependent spectrum of various types of reversible contractile dysfunction as a function of myocardial flow reserve and resting MBF. The spectrum proceeds from normal to scar tissue or loss of viability. As the coronary flow reserve declines, occasional episodes of ischemia and stunning lead to intermittent dysfunction of stunning associated with enhanced glucose uptake. More severe reductions in flow reserve are then associated with repetitive ischemia and repetitive stunning leading to chronically reduced contractile function but increased glucose uptake. With progression of the coronary artery stenosis, resting MBF may decline, while the increased glucose uptake is maintained until the amount of fibrosis increases and more myocytes undergo necrosis and metabolic activity ceases energy requirements match the available energy supply. A new supply-demand imbalance is established, but at a lower level. Such a new balance, however, will be a precarious one because even moderate increases in demand or decreases in supply disturb the steady state and cause ischemia. It is thus possible and likely that both hibernation and stunning coexist to varying extents in many patients. Observations in experimental animals suggest that sustained reductions in both blood flow and contractile function can be maintained for some time without significant necrosis, but development of structural alterations resembling those in patients with chronic CAD supports the concept of hibernation.