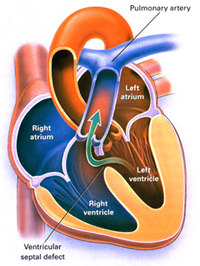
Ventricular Septal Defect (VSD) is the most
common congenital heart abnormality in infants and children,
with equal frequency in both sexes.
25-40% of these defects close
spontaneously by the age of two; 90% of those which close eventually
do so by the age of ten. 70% are located in the membranous part
of the interventricular septum (IVS) close to the pulmonary
valves and artery, 20% in the muscular portion of the IVS (see
figures
104b,
105a), 5% just below the aortic valve (causing regurgitation),
and 5% near junction of mitral and tricuspid valves (atrioventricular
canal defects).
The consequences of a VSD depend on the size
of the defect and the relative resistance in aortic and pulmonary
artery beds. A small defect causes little disturbance, as the
unequal increase in pulmonary blood flow is minimal.
But if the defect is large, the ventricular
pressures (right and left) are equal and the size of flow into
the pulmonary and aortic, systemic (remainder of body) circulations
is determined by the resistances in the two beds.
At first, the systemic, aortic resistance
is greater than in the pulmonary, so the shunt of blood is left
to right (see figure 112c). In
time the pulmonary resistance increases, and the size of the
left to right shunt decreases. When the pulmonary resistance
equals or exceeds that in the aortic system, the shunt changes
from left to right, to right to left.