PSVT
due to accessory pathways ( PSVT. The mechanism of the tachyarrhythmia relates to the presence of two pathways between the atria and the ventricles
)
This
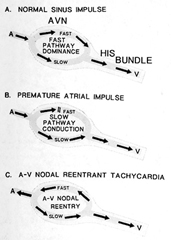
syndrome is the second most common cause of PSVT. The mechanism
of the tachyarrhythmia relates to the presence of two pathways
between the atria and the ventricles that have different conducting
properties (see figure1).
Usually the period of these pathways during
which they can not respond to stimulus to conduct (refractory
period) exceeds that of the normal AV nodal-His pathway. Thus,
a premature atrial impulse may block at the accessory pathway
and conduct antegrade down the normal pathway and enter the
accessory one in a retrograde direction and reentering the atrium
to cause a circus movement tachycardia (orthodromic, see figure
3).
Since
the accessory pathway provides retroconduction to the atria,
P waves (if seen) are usually inverted in EKG leads like AVF
and V5-6.
Less
common is for the accessory pathway to have a shorter refractory
period causing a block of an initiating premature atrial impulse
in the normal pathway, with antegrade conduction down the anomalous
pathway and retrograde invasion of the normal AV node pathway
to establish an antidromic tachycardia (see figure 3) with wide
QRS's in the EKG. These wide QRS tachycardias may be difficult
to distinguish from VT if the existence of WPW was not known
prior to presentation with a tachyarrhythmia. In concealed WPW
syndrome, only orthodromic tachycardias can occur because of
the inability of the bypass tract to conduct in the antegrade
direction. Distinction between concealed WPW and AV nodal reentrant
tachycardia may be difficult, although a faster rate (>200
per minute) and a retrograde P wave after, rather than within,the
QRS complex favor concealed WPW.When atrial flutter or fibrillation
occur in patients with WPW, the risk of potentially lethal arrhythmias
due to very rapid conduction across accessory pathways
must be considered. The risk is especially treacherous in patients
with short-refractory period anomalous pathways, since atrial
fibrillation may lead to ventricular fibrillation.
Reference:Myerburg,R.J.
and others,Hurst's The HEART,8TH Edition,Recognition Clinical
Assessment,and Management of Arrhymthmias and Conduction Disturbances,Ch.36,pp.705-758
PSVT's can be classified into two major groups:short RP and
long RP tachycardias, that is the P wave during the SVTs occurs
either in the first or second half of the tachycardia cycle.Since
the PR interval is inversely related to the RP interval,short
RP tachycardias have long PR intervals,and long RP intervals
have short PR intervals.
These
SVTs are defined by having atrial activity:
1) obscured by the QRS complex because
ofthe simultaneous inscription of both,
2) occurring in the terminal portion of the QRS complex and
often giving the appearance of an R' in lead V1. or
3) present in the STsegment.
Thus, the interval from the onset of the QRS to the P wave is
short--"short RP SVT". The most likely SVT for the
first and second examples is atrioventricular nodal pathway
reentrant tachycardia (AVNRT), using the slow AV nodal pathway
anterogradely and the fast AV nodal pathway retrogradely. An
SVT traveling to the ventricle over the AV node and back to
the atrium over an accessory pathway, called "atrioventricular
reentrant tachycardia" (AVRT; WPW), is the most likely
cause of the third example, and less commonly the second.
Important
data can help refine the diagnosis if a functional bundle branch
block (FBBB) also occurs. Prolongation of the SVT cycle length
during FBBB is most consistent with an AVRT and the location
of the accessory in the same ventricle that gave rise to the
FBBB. Thus prolongation of the SVT cycle length during a period
of a functional left BBB (LBBB) would be found during AVRT due
to retrograde conduction over a left- sided accessory pathway;
the same analysis applies to functional right BBB (RBBB) and
right-sided accessory pathway.The cycle length prolongs because,during
the FBBB,the antegrade impulse must first activate the ventricle
contralateral to the ventricle with the FBBB. Failure of the
FBBB to prolong the cycle length of the AVRT occurs when the
accessory pathway is located contralateral to the ventricle
with the FBBB, in many AVRTs due to septal accessory pathways,
and non-WPW forms of SVT.EKG algorithms based on the form of
the delta wave of the WPW complex can be used to determine the
location of the accessory pathway.
These
are characterized by atrial activity locatd "just before"
the next QRS complex,so that the P wave is located in the second
half of the tachycardia cycle at a conductible PR interal of
approximately 300ms. or so. This SVT creates a long interval
from the preceding QRS complex to the next P wave. This type
is typical of atrial tachycardia and two other SVTs. One is
an unusual form of AVRT comprised of a slowly conducting accessory
pathway that creates an incessant SVT, which pauses briefly
for a few sinus beats and then resumes (called junctional reciprocating
tachycardia, PJRT) and because of its incessant nature can cause
a tachycardia cardiomyopathy. The impulse travels over the normal
conducting system and then back over the slow-conducting accessory
pathway. The third type of long RP SVT is an unusual form of
AVNRT, during which the impulse travels to the ventricle over
the fast-conduction pathway, and retrogradely over the slow-conducting
pathway (the reverse route traveled by the usual type of AVNRT).
| Intermittent
RP Tachycardia |
Several
infrequently occurring SVT's can give rise to tachycardias that
have PR and RP intervals of about the same duration so that
the P wave is found midway in the tachycardia cycle. They include
AVNRT when the impulse travels over two slowly conducting pathways,
unusual forms of AVRTs, and some atrial tachycardias.
| Spontaneous
Onset Or Termination of The SVT |
A
sustained SVT initiated by a premature atrial complex(PAC) causing
block in an accessory pathway is most likely an AVRT, where
as a sustained SVT started by a PAC that significcantly prolongs
the PR interval is probably AVNRT. An SVT always stopping with
a P wave rather than a QRS complex as the electral event last
inscribed in the EKG is unlikely to be an atrial tachycardia,
because the atrial focus would always have to block en route
to the ventricle at the same time it stopped discharging, unlikely
set of coincidences to happen repeatedly. Far more likely is
either AVNRT or AVRT, during which atrial activity blocks before
reaching the ventricle, thus interrupting the reentrant loop
and terminating the tachycardia. Similarly, an SVT that persist
uninterruptedly despite blocked P waves is almost certainly
an atrial tachycardia,rarely AVNRT, and never the usual forms
of AVRT.
Reference:Zipes,D.P.,Clinical
Application of the EKG,JACC,Vol.36,No.6,2000:1746-8
Management of PSVT due to WPW syndrome includes: adenosine,
verapamil, diltiazem, pronestyl, and quinidine,which may be
used to convert the acute tachycardia to normal. Digoxin is
to be avoided to prevent shortening of refractory period of
accessory pathway as well as atrial muscle. Electrical cardioversion
may be used if drug therapy fails. Catheter ablation can be
used for life threatening arrhythmias in WPW (atrial
fibrillation, see figures 1b, 3b).
Surgery can be used
if ablation therapy is unsuccessful.
Reference:Myerburg,R.J.
and others,Hurst's The HEART,8TH Edition,Recognition Clinical
Assessment,and Management of Arrhymthmias and Conduction Disturbances,Ch.36,pp.705-758
Wolff-Parkinson-White Syndrome
Last Updated: September 5, 2002
Author: Vibhuti N Singh, MD, MPH, FACC
, Director, Heart Center of St Petersburg; Clinical Assistant
Professor, Department of Internal Medicine, Division of Cardiovascular
Disease, University of South Florida College of Medicine
Coauthor(s): Rakesh K Sharma, MD, FACC, FACP,
Interventional Cardiologist, The Heart and Vascular Institute
of Florida; Greg Flaker, MD, FACC, Professor of Medicine, Director,
Division of Cardiology, University of Missouri at Columbia Health
Sciences Center
Vibhuti N Singh, MD, MPH, FACC, is a member
of the following medical societies: American College of Cardiology,
American College of Physicians, American Heart Association,
American Medical Association, and Florida Medical Association
INTRODUCTION
Background: Wolff-Parkinson-White (WPW) syndrome
is a congenital abnormality associated with supraventricular
tachycardia (SVT). It involves an activation of the ventricles
that occurs earlier than expected, called preexcitation, which
occurs because of conduction of an atrial impulse not by means
of the normal conduction system, but via an extra atrioventricular
(AV) muscular connection, termed an accessory pathway, that
bypasses the AV node.
Classic ECG findings of WPW syndrome include
a short PR interval (<120 ms), a wide QRS complex of longer
than 120 milliseconds with a slurred onset producing a delta
wave in the early part of QRS, and secondary ST-T wave changes.
Patients with WPW syndrome are potentially
at an increased risk of dangerous ventricular arrhythmias due
to extremely fast conduction across the bypass tract if they
develop atrial flutter or fibrillation. Certain patients with
WPW syndrome are at risk for sudden death. In these patients,
cardiac electrophysiologic (EP) studies and radiofrequency (RF)
catheter ablation may be curative. Other patients have symptomatic
SVT, which can also be cured by catheter ablation. Asymptomatic
patients may merely need periodic observation.
This review discusses the pathogenesis, clinical
presentation, evaluation, and treatment of patients with WPW
syndrome.
Pathophysiology: Patients with preexcitation
may have SVT due to a reentrant mechanism. The genesis of reentrant
SVT involves the presence of dual conducting pathways between
the atria and the ventricles. These pathways include (1) the
natural AV nodal His-Purkinje tract and (2) an AV accessory
tract (ie, AV connection or bypass tract, Kent fibers, or Mahaim
fibers.
The 2 pathways usually exhibit 2 different
conduction properties and refractory periods that facilitate
reentry. The effective refractory period (ERP) of the accessory
tract is usually longer than that of the normal AV nodal His-Purkinje
tract. Several types of SVT have been described, including orthodromic
tachycardias, orthodromic tachycardia with a concealed accessory
pathway, and antidromic tachycardia.
Orthodromic tachycardia
When a premature ectopic atrial impulse begins
to traverse down towards the ventricle, it may block at the
accessory tract but conduct in antegrade fashion down the normal
pathway. The impulse then reenters the accessory tract in retrograde
fashion to perpetuate a circus movement of the impulse. Such
reentrant tachycardia is described as orthodromic. Premature
ventricular contractions (PVCs) can also initiate orthodromic
tachycardia.
In orthodromic tachycardia, the normal pathway
is used for ventricular depolarization and the accessory tract
is used for reentry. On ECG findings, the delta wave is absent,
QRS complex is normal, and P waves are inverted in the inferior
and lateral leads.
Orthodromic tachycardia with a concealed accessory
pathway
Some accessory (bypass) tracts are unable
to conduct in the antegrade fashion. These are called concealed
accessory pathways (ie, concealed WPW syndrome). Although no
evidence of the pathway is present during sinus rhythm (ie,
no preexcitation), orthodromic tachycardias can occur.
Differentiation between this type of SVT and
usual AV nodal reentrant tachycardia (AVNRT) may be difficult.
Nonetheless, if the heart rate is higher than 200 beats per
minute and a retrograde P wave is visible following the QRS
complex, a concealed accessory pathway may be the diagnosis.
Antidromic tachycardia
Less commonly, a shorter refractory period
in the accessory tract may cause block of an ectopic atrial
impulse in the normal pathway, with antegrade conduction down
the accessory tract and then retrograde reentry of the normal
pathway. This type of tachycardia produced is called antidromic
tachycardia.
On ECG findings, the QRS is wide, which is
an exaggeration of the delta wave during sinus rhythm (ie, wide-QRS
tachycardia). Such tachycardias are difficult to differentiate
from ventricular tachycardia.
Thus, the mechanism underlying the majority
of the tachycardias in patients with WPW syndrome is macroreentry
caused by antegrade conduction over the AV node His bundle pathway
and retrograde conduction over an accessory pathway (orthodromic).
Less common in patients with WPW syndrome is antidromic tachycardia.
Even when the accessory pathway conducts only in retrograde
fashion, it can still participate in the reentrant circuit and
produce an orthodromic AV reciprocating tachycardia.
Frequency:
In the US: The prevalence of ventricular
preexcitation is thought to be 0.1-0.3% in the general population.
Estimates of arrhythmia incidence in patients with preexcitation
vary widely, ranging from 12-80% in several surveys.
Incidence of preexcitation and WPW syndrome
varies from 0.1-3 cases per thousand population (average of
1.5 cases per thousand population) in otherwise healthy persons.
In a review of ECG findings from 22,500 healthy
aviation personnel, 0.25% exhibited findings consistent with
the WPW pattern, with 1.8% incidence of tachycardia.
The location of the accessory pathways, in
descending order of frequency, is (1) the left free wall, (2)
posteroseptal, (3) right free wall, and (4) anteroseptal.
The presence of concealed accessory pathways
accounts for approximately 30% of patients with apparent SVT
referred for EP evaluation.
Approximately 80% of patients with WPW syndrome
have a reciprocating tachycardia, 15-30% have atrial fibrillation,
and 5% have atrial flutter. Ventricular tachycardia is uncommon.
Internationally:
Incidence and prevalence of WPW syndrome
worldwide parallels that in the United States.
Mortality/Morbidity:
Patients with WPW syndrome have a very small
risk of sudden arrhythmic death. Medical therapy with agents
such as digoxin may increase this risk. The risk in asymptomatic
patients is extremely low.
Overall, sudden death occurs rarely, with
an estimated frequency rate of 0.1%.
Other factors that appear to influence risk
are the presence of multiple bypass tracts and a family history
of premature sudden death. Sudden cardiac death is unusual without
preceding symptoms.
Race: No clear
racial predilection appears to exist.
Sex: Prevalence
may be higher in males.
Age: Certain
factors exist regarding age and the prevalence of preexcitation
and WPW syndrome.
WPW syndrome is found in persons of all ages,
from those in fetal and neonatal age groups to elderly individuals.
Prevalence decreases with age because of
loss of preexcitation. Cases have been described in which electrocardiographic
evidence of preexcitation disappears.
In patients with abnormal ECG findings indicative
of WPW syndrome, the frequency of SVT paroxysms increases from
10% in people aged 20-39 years to 36% in people older than 60
years.
CLINICAL
History:
WPW syndrome can result in SVT that uses
an AV accessory (bypass) tract. The accessory pathway may also
act as an innocent bystander and allow conduction during other
supraventricular arrhythmias, such as atrial fibrillation or
flutter. The possibility of a concealed bypass tract as a mechanism
underlying certain types of SVT should be considered because
treatment options may vary. Paradoxically, the use of digoxin
and perhaps other AV nodal blocking agents may accelerate conduction
through the bypass tract, causing potentially lethal ventricular
arrhythmias or hemodynamic instability during atrial fibrillation.
SVT in WPW syndrome may begin in childhood
or not appear clinically until the patient reaches middle age.
In some patients in whom it first presents during childhood,
it may then cease for some time, only to recur. In fact, the
probability is 75% that the tachycardia will persist if it is
still present in patients older than 5 years.
In asymptomatic patients, the probability
of losing the capacity for antegrade conduction across the accessory
pathway increases with advancing age. This probably results
from fibrotic changes at the site of insertion of the accessory
bypass tract.
In patients with WPW syndrome, the tachycardia
that produces symptoms may be an SVT, atrial fibrillation, or
atrial flutter. In a series of 212 patients with tachyarrhythmias
and WPW syndrome, SVT alone occurred in 64%, atrial fibrillation
alone in 20%, and both occurred in 16% of patients.
Light-headedness and near syncope appear
to occur more commonly in persons with WPW syndrome who have
paroxysmal SVT (PSVT) or atrial fibrillation than in those with
AV nodal reentry.
Syncope can occur because of inadequate cerebral
circulation due to a rapid ventricular rate or because the tachyarrhythmia
is depressing the sinus pacemaker, causing a period of asystole
at the point of tachycardia termination.
PSVT can be followed after termination by
polyuria, which is due to atrial dilatation and release of atrial
natriuretic factor.
Physical:
During SVT, the rhythm is unvarying and regular,
with constant intensity of the first heart sound.
The jugular venous pressure can be elevated,
but the waveform generally remains constant.
Clinical features of associated cardiac defects
may be present, such as the following:
Mitral valve prolapse
Cardiomyopathy
Ebstein anomaly: Patients with right-sided
accessory pathways should be screened for the Ebstein anomaly.
The abnormal QRS complexes of WPW syndrome,
when present, may appear similar to those observed in acute
myocardial infarction (MI). Repolarization abnormalities are
common in patients with WPW syndrome.
Causes: In patients with WPW syndrome, the
underlying cardiac structural abnormality consists of accessory
conduction tissue that bypasses the normal AV node His-Purkinje
system pathway. Such pathways are generally believed to be
congenital in nature.
The causes of WPW syndrome can be summarized
as follows:
Congenital or hereditary
An accessory pathway is quite likely to
be congenital, although its manifestations can be detected
in later years and it may appear to be acquired.
Relatives of patients with preexcitation,
particularly those with multiple pathways, have an increased
prevalence of preexcitation, suggesting a hereditary mode
of acquisition.
Associated with congenital cardiac defects
Patients with the Ebstein anomaly may develop
WPW syndrome. Patients with the Ebstein anomaly frequently
have multiple accessory bypass tracts, mostly right-sided,
in the posterior part of the septum or the posterolateral
wall. Preexcitation generally occupies the atrialized ventricle.
The orthodromic reciprocating tachycardia in such patients
exhibits right bundle-branch block (RBBB) and a long ventriculoatrial
(VA) interval.
Mitral valve prolapse may be a congenital
cardiac defect and may cause WPW syndrome.
Hypertrophic cardiomyopathy may include
idiopathic hypertrophic subaortic stenosis or asymmetric septal
hypertrophy.
Associated with other acquired cardiac
defects - Cardiomyopathies
DIFFERENTIALS
Atrioventricular Nodal Reentry Tachycardia (AVNRT)
Ebstein Anomaly
Lown-Ganong-Levine Syndrome
Syncope
Other Problems to be Considered:
In Lown-Ganong-Levine (LGL) syndrome, patients
have a short PR interval and SVT, but no delta wave.
Mahaim fibers connect the atria to the right
bundle or the AV node to the ventricle. Such bypass tracts are
called atriofascicular. If atriofascicular fibers are present,
the ECG findings are a normal or short PR interval and the QRS
complex is abnormally wide with a left-bundle appearance. These
fibers have decremental conduction properties and can perpetuate
clinically significant tachycardias or act as innocent bystanders
for other types of tachycardias (eg, AVNRT).
Sometimes, the fibers arise in the His bundle
or bundle branches and insert into the ventricular myocardium.
These are called fasciculoventricular tracts and, generally,
are not involved in tachycardias.
Differential diagnosis of accessory pathway
syndromes using EP studies
In patients with LGL syndrome who have an
atriohisian tract, the QRS complex remains normal and the short
atriohisian interval remains fixed during atrial pacing at rapid
rates.
Patients with fasciculoventricular connections
show a short His-ventricle (HV) interval and no change in the
QRS complex during rapid atrial pacing.
Atriofascicular tract pathways usually represent
a duplication of the AV node and the distal conducting system.
They occupy the right ventricular free wall. Their proximal
end resides adjacent to the lateral tricuspid annulus and exhibits
slow conduction, with AV nodelike characteristics. The distal
end, which conducts rapidly, inserts into the distal right bundle
branch or the apical region of the right ventricle. Preexcitation
may not be apparent during sinus rhythm but can be demonstrated
with premature right atrial stimulation. Because retrograde
conduction is absent, only an antidromic AV reentry tachycardia
(ie, preexcited tachycardia) can develop.
Furthermore, concerning atriofascicular tracts,
preexcited tachycardia has a left bundle-branch block pattern,
long AV interval (due to the long conduction time over the accessory
pathway), and short VA interval. If RBBB develops, it can become,
by increasing the length of the tachycardia circuit (ie, VA
interval prolongs owing to delay in retrograde activation of
the His bundle), proarrhythmic and the tachycardia can become
perpetual and persistent.
Patients with PSVT usually have narrow QRS
complexes. The QRS may become wider owing to aberrant conduction,
coexisting bundle-branch block, or involvement of an accessory
pathway.
Other forms of tachycardia in patients with
WPW syndrome
Patients with WPW syndrome can have other
tachycardias during which the accessory pathway is just a bystander,
such as AVNRT or an atrial tachycardia that conducts to the
ventricle over the bypass tract.
Atrial flutter or fibrillation may also occur
in the atrium, unrelated to the bypass tract.
Patients with WPW syndrome who have atrial
fibrillation frequently have inducible reciprocating tachycardias.
Interruption of the accessory pathway with ablation can prevent
recurrence of the atrial fibrillation.
Atrial fibrillation presents a potentially
serious risk. At rapid rates, the refractory period of the accessory
pathway can shorten, allowing an exceedingly rapid ventricular
response. However, such a phenomenon is uncommon, occurring
at an estimated frequency of less than 0.1%.
Patients who have intermittent preexcitation
or those who lose ECG evidence of preexcitation with exercise
or when injected intravenously with procainamide generally have
a long refractory period of the bypass tract. These patients
are thought to have a low risk of developing a rapid ventricular
rate should atrial flutter or fibrillation develop.
Atrioventricular Nodal Reentry Tachycardia (AVNRT)
Ebstein Anomaly
Lown-Ganong-Levine Syndrome
Syncope
WORKUP
Lab Studies:
Routine blood studies may be needed to help
rule out noncardiac conditions triggering tachycardia. These
may include the following:
Complete blood cell count
Chemistry panel
Blood urea nitrogen and creatinine to assess
renal status
Liver function tests (eg, bilirubin and
transaminase levels)
Thyroid panel
Blood levels of antiarrhythmic medications
during therapy and monitoring
Imaging Studies:
Echocardiogram may be needed to assess
left ventricular function and wall motion and to help rule
out valvular disease, Ebstein anomaly, hypertrophic cardiomyopathy
(in which the incidence of accessory pathways is increased),
or other congenital cardiac defects.
Other Tests:
The diagnosis and management of any
cardiac arrhythmia can be accomplished by using findings from
ECG and rhythm strip analysis and their relationship to the
clinical setting. Recognizing arrhythmias on ECG findings
requires a thorough knowledge of atrial and ventricular activation
patterns and deductions related to the mechanisms of AV conduction.
The standard 12-lead ECG and additional
rhythm strips form a direct and easily accessible resource
for analyzing abnormalities of the cardiac rhythm. For many
simple arrhythmias, mere recognition of P-wave and QRS morphologies,
with their relative timing and their vectors, may be sufficient
to confirm a diagnosis.
The location of the accessory pathway using
ECG can often be determined by a thorough analysis of the
spatial direction of the delta wave in the 12-lead ECG findings
by reviewing the maximally preexcited QRS complexes.
Ladder diagram of the ECG
Analysis of more complex arrhythmias may
require the use of ladder diagrams or Lewis lines (named after
Sir Thomas Lewis, who first used them).
The ladders usually consist of 3 tiers:
A, AV, and V. Additional tiers, such as sinoatrial (SA) conduction,
may be added. The A and V tiers correspond to the activation
of atrial (A) and ventricular (V) muscle.
AV is used to show conduction in the AV
junction. The A line is drawn from the beginning of the P
wave, and the V line is drawn from the beginning of the QRS.
Time is indicated by the slope of the line.
The site of origin may be represented by
a black dot.
A blocked impulse is indicated by a short
bar at a right angle to the line, indicating the direction
of conduction, and aberrant intraventricular conduction is
shown as a pair of slightly divergent lines.
Special ECG leads
When the standard ECG fails to provide
adequate information to support a diagnosis, often because
of a failure to recognize P waves, certain additional special
lead systems can be used to help establish the diagnosis.
A bipolar esophageal lead is used to record
left atrial activity, while an intra-atrial electrode during
catheterization can be used to record atrial activity from
within the right atrium.
Continuous ECG recordings (ie, telemetry,
24-hour Holter monitor, event monitor, implantable loop recorder)
Continuous monitoring of cardiac rhythm
can be performed on hospitalized patients in the coronary
or the progressive care units with telemetry.
In the outpatient setting, a number of
portable recording devices (eg, Holter monitors, event monitors)
can be used.
Portable recording systems provide simultaneous
2-lead recording that improves the diagnostic yield tremendously.
The 2 most commonly used leads for monitoring are lead II
and MCL-I, the latter being similar to V1. These devices have
long-term storage capabilities that permit off-line analysis
of complex arrhythmias, even if the physician is not available
at the time the rhythm disturbance occurs.
For infrequently occurring arrhythmias,
a number of event recorders are available. They allow the
patient to activate the device by pressing a button when an
event occurs, providing internal storage and transmission
by telephone or wireless communication to a central station
for later review.
Transtelephonic transmitters can be used
in real time for somewhat more persistent or frequent events.
A small loop recorder can be implanted
similar to a pacemaker and can be removed later for analysis.
This can be used in patients with arrhythmias that are difficult
to capture.
ECG recognition of reentry over a retrograde
(concealed) accessory pathway
A bypass tract that conducts unidirectionally
only from the ventricle to the atrium is not detectable on
the regular surface ECG findings because the ventricle is
not preexcited; thus, the ECG manifestations of WPW syndrome
are absent.
Such a bypass tract is described as concealed.
Tachycardia due to the concealed tract
should be considered when the QRS complex is normal and the
retrograde P wave occurs well after completion of the QRS
complex, out in the ST segment or even in the T wave.
Diagnosis of accessory pathways
During ventricular pacing, premature ventricular
stimulation activates the atria before retrograde depolarization
of the His bundle. This indicates that the impulse reached
the atria before it depolarized the His bundle and must have
traveled a different pathway (bypass tract).
If the ventricles can be stimulated prematurely
during tachycardia at a time when the His bundle is refractory
and the impulse still conducts to the atrium, this indicates
that retrograde propagation traveled to the atrium over a
pathway other than the bundle of His.
If the premature ventricular complex depolarizes
the atria without lengthening of the VA interval and with
the same retrograde atrial activation sequence, the stimulation
site (ie, ventricle) may be assumed to be within the reentrant
circuit without intervening His-Purkinje or AV nodal tissue
that might increase the VA interval and therefore the AA interval.
In addition, if a premature ventricular
complex delivered at a time when the His bundle is refractory
terminates the tachycardia without retrograde activation of
the atria, it most likely invaded, and blocked in, an accessory
pathway.
The VA interval (a measurement of conduction
over the accessory pathway) is generally constant over a wide
range of ventricular paced rates and coupling intervals of
premature ventricular complexes and during the tachycardia
in the absence of aberration. Similar short VA intervals can
be observed in some patients during AV nodal reentry, but
if the VA conduction time or R-P interval is the same during
tachycardia and ventricular pacing at comparable rates, an
accessory pathway is almost certainly present. The VA interval
is usually less than 50% of the R-R interval.
Tachycardia can be initiated easily following
premature ventricular stimulation that conducts in retrograde
fashion in the accessory pathway but blocks in the AV node
or His bundle. Atria and ventricles are required components
of the macroreentrant circuit; therefore, continuation of
the tachycardia in the presence of AV or VA block excludes
an accessory AV pathway as part of the reentrant circuit.
Stress testing
This is an ancillary test and may be used
to (1) reproduce a transient paroxysmal arrhythmia, (2) document
the relationship of exercise to the onset of tachycardia,
(3) evaluate the efficacy of therapy, and (4) assess adverse
responses.
A bicycle ergometer or standard treadmill
can be used.
Thallium or echocardiographic imaging is
not necessary unless an ischemic etiology is considered as
a potential cause or trigger of the onset of arrhythmia.
Stress testing may also provide some general
insight into the refractory periods of accessory pathways
in patients with WPW syndrome.
Procedures:
Intracardiac EP studies
EP studies are performed in a cardiac electrophysiology
laboratory. Using multicatheter electrode systems, recordings
from many intracardiac sites can be performed simultaneously,
facilitating delineation of the sequence of depolarization
and impulse conduction in the atria, AV junction, and ventricle.
EP studies can be used in patients with
WPW syndrome to determine (1) the mechanism of the clinical
arrhythmia, (2) EP properties (eg, conduction capability,
refractory periods) of the accessory pathway and the normal
conduction system, (3) the number and location of accessory
pathways (which is necessary for catheter ablation), and (4)
the response to pharmacological or ablation therapy.
Indications for EP studies in patients
with WPW syndrome according to the American College of Cardiology/American
Heart Association guidelines
Class I indications include (1) patients
being evaluated for catheter ablation or surgical ablation
of an accessory pathway, (2) patients with ventricular preexcitation
who have survived cardiac arrest or who have unexplained syncope,
and (3) symptomatic patients in whom determination of the
mechanism of arrhythmia or knowledge of the EP properties
of the accessory pathway and normal conduction system would
help in determining appropriate therapy.
Class II indications include (1) asymptomatic
patients with a family history of sudden cardiac death or
with ventricular preexcitation but no spontaneous arrhythmia
who engage in high-risk occupations or activities and in whom
knowledge of the EP properties of the accessory pathway or
inducible tachycardia may help determine recommendations for
further activities or therapy and (2) patients with ventricular
preexcitation who are undergoing cardiac surgery for other
reasons.
Class III indications include asymptomatic
patients with ventricular preexcitation, except those in class
II.
EP features of preexcitation
If a Kent bundle (AV)–type accessory
bypass tract conducts in an antegrade fashion, 2 parallel
paths can potentially carry the impulse. The first is the
natural one, which comes with inherent physiological delay
over the AV node. The second is the bypass tract (Kent bundle),
which allows the impulse to pass directly without delay from
the atrium to the ventricle.
This dual-path mechanism produces a unique
QRS complex that is a form of fusion beat due to depolarization
of the ventricle from these 2 pathways.The delta wave results
from ventricular activation by the impulse traveling over
the accessory pathway.
The extent of contribution to ventricular
depolarization by the wavefront over each route varies, as
follows:
If delay in AV nodal conduction occurs
from either rapid atrial pacing or a premature atrial complex,
a greater proportion of the ventricle activates via the bypass
tract and the QRS becomes more abnormal in shape.
On the other hand, if the bypass tract
is far from the sinus node (as in the presence of a left lateral
pathway) or if AV nodal conduction is rapid, a larger proportion
of the ventricle activates via the normal pathway.The normal
fusion beat during sinus rhythm has a short or negative HV
interval. This occurs because the His bundle activation begins
later than the ventricular activation from the bypassing impulse,
while the impulse traveling over the AV node just reaches
the His bundle. Pacing the atrium rapidly at premature intervals
accentuates the abnormal ventricular depolarization and further
shortens the HV interval.
Recognition and localization of accessory
pathways using EP studies
When retrograde atrial activation during
tachycardia occurs over an accessory pathway that connects
the left atrium to the left ventricle, the earliest retrograde
activity is recorded from a left atrial electrode (usually
positioned in the coronary sinus). This is a left lateral
pathway.
When retrograde atrial activation during
tachycardia occurs over an accessory pathway that connects
the right ventricle to the right atrium, the earliest retrograde
atrial activity is generally recorded from a lateral right
atrial electrode. This is a right ventricular free wall pathway.
Participation of a septal accessory pathway
creates earliest retrograde atrial activation in the low-right
atrium situated near the septum, anterior or posterior, depending
on the insertion site.
Mapping techniques with intravenous catheter
electrodes placed at the time of surgery may help provide
accurate assessments of the position of the accessory pathway.
Recording electrical activity directly from the accessory
pathway obviously provides the most precise localization.
Retrograde atrial activation over the accessory
pathway on EP studies
This can be confirmed by inducing premature
ventricular complexes during tachycardia to determine whether
retrograde atrial excitation can occur from the ventricle
at a time when the His bundle is refractory.
Because VA conduction cannot occur over
the normal conduction system because the His bundle is refractory,
an accessory pathway must be present for the atria to become
excited and most likely is participating in the tachycardia
circuit.
The following parameters may be helpful:
Patients with a reciprocating tachycardia
due to an accessory AV bypass tract almost always have a VA
interval of greater than 70 milliseconds measured from the
onset of ventricular activation to the onset of atrial activity
recorded on an esophageal lead or greater than 95 milliseconds
when measured to the high-right atrium.
In contrast, in most patients with AVNRT,
the interval from the onset of ventricular activity to the
earliest onset of atrial activity is characteristically shorter
than 70 milliseconds.
Intraoperative (multiarray) epicardial
mapping and endocardial catheter mapping using EP studies
Mapping of the pathways and sites of origin
for both ventricular and supraventricular tachyarrhythmias
has led to tremendous improvements in surgical outcomes, which
has given way to catheter techniques for ablation procedures.
Multiple electrode arrays allow simultaneous
recordings from several intracardiac sites during the same
cardiac cycle, generating maps of wave activation. This technology
allows the clinical electrophysiologist and surgeon to identify
target areas for surgical ablation.
Although quite successful in prior years,
intraoperative mapping for WPW syndrome has now been replaced
by catheter mapping during EP studies and ablation procedures.
Histologic Findings: Histologic findings
of accessory bypass pathways have been described with careful
dissection of the AV space.
TREATMENT
Medical Care: Treatment of arrhythmia is directed
at the underlying cause and the triggers that perpetuate the
arrhythmia. The underlying cause includes primary arrhythmias
due to an EP abnormality resulting from definable structural
heart disease and occurring independently of hemodynamic or
metabolic disturbance. Such arrhythmias include coronary heart
disease, ischemia, cardiomyopathy, pericarditis, and WPW syndrome.
The triggers that perpetuate the arrhythmia include secondary
arrhythmias, such as electrolyte imbalance, metabolic defects,
and hemodynamic and hypoxemic abnormalities.
Appropriate treatment of WPW syndrome is based
on its likely prognosis. Patients with only ECG evidence of
preexcitation, without documented episodes of tachyarrhythmias,
generally do not require either aggressive workup through EP
studies or treatment with antiarrhythmic agents.
The 3 main treatment modalities for WPW syndrome
are drug therapy, electrical (ie, RF) ablation, and surgical
ablation. Ablation is the first-line treatment for symptomatic
WPW syndrome. It has replaced surgical treatment and most drug
treatment. However, drug therapy can be useful in some instances,
such as in patients who refuse ablation or in patients in whom
ablation fails in one or two attempts. For patients treated
longitudinally with pharmacotherapy, consideration should be
given to a membrane-active antiarrhythmic drug (class IC or
III) with an AV nodal blocker, rather than just an AV nodal
blocker, because of the potential for extremely rapid rates
during preexcited atrial fibrillation or flutter
Drug therapy (potential antiarrhythmic mechanisms):
Antiarrhythmic drugs act on the AV node (ie, AV node blocking
agents), myocardial tissue, and/or the accessory pathways. They
work by increasing the refractory period or by prolonging the
conduction time to prevent perpetuation of an AV reciprocating
tachycardia. They may also act to reduce the ventricular response
to atrial flutter or atrial fibrillation.
AV node blocking drugs
Adenosine, verapamil, metoprolol, and digitalis
all prolong conduction time and refractoriness in the AV node.
Verapamil and metoprolol do not affect conduction
in the bypass tract.
Digitalis exhibits variable effects and may
even shorten the refractory period.
None of these drugs should be given in an
acute phase to a patient with ventricular preexcitation who
has atrial fibrillation.
Digoxin is contraindicated in patients with
WPW syndrome, although it may play some role in children only.
Most deaths from WPW syndrome have been associated with digoxin
use.
Propranolol is almost never administered.
Metoprolol or atenolol can be useful in some patients.
Agents affecting the accessory pathways
Class IA drugs (eg, procainamide) and class
IC drugs (eg, flecainide, propafenone) block conduction in the
accessory pathway.
Amiodarone and sotalol influence both the
AV node and the bypass tract. They work in similar fashion but
affect only the bypass tract.
Class IA and IC drugs that prolong the refractory
period in the bypass tract are indicated if drug therapy becomes
necessary.
Class IC and IA drugs are best used in conjunction
with an AV node blocker, such as metoprolol or verapamil.
Procainamide and quinidine are relics of
the past for long-term treatment.
Caution when treating WPW syndrome tachycardia
Digitalis shortens refractoriness in the
myocardium and in the bypass tract. Thus, it may accelerate
the ventricular response in the setting of atrial fibrillation
in a patient with WPW syndrome. Adenosine should not be used
in this setting.
Digitalis should not be used in such patients,
except perhaps in pediatric or elderly patients. Instead, medicines
that prolong the refractory period in the accessory pathway
(eg, class IA and IC agents) should be used.
Intravenous verapamil can likewise speed
up the ventricular response in patients with WPW syndrome who
have atrial fibrillation. This does not appear to happen with
oral verapamil. Verapamil is not recommended as a sole agent
in patients with WPW syndrome.
Termination of an acute episode
Narrow-complex AV reentrant tachycardia
Such tachycardias manifest with normal QRS
complexes, a ventricular rate of more than 200 beats per minute,
regular R-R intervals, and a retrograde P wave well beyond the
end of QRS.
They should be treated in the same way as
AVNRT, by blocking AV node conduction with (1) vagal maneuvers
(eg, Valsalva maneuver, carotid sinus massage, splashing cold
water or ice water on the face), (2) intravenous adenosine,
or (3) intravenous verapamil or diltiazem (ie, if recurrent
SVT is present, if adenosine is ineffective, or if the patient
is taking theophylline).
Note that atrial fibrillation can occur after
drug administration, particularly adenosine, with a rapid ventricular
response. An external cardioverter-defibrillator should be immediately
available in case it is necessary.
Atrial flutter/fibrillation or wide-complex
tachycardia
Atrial flutter/fibrillation can be recognized
by the presence of abnormal QRS complexes and irregular R-R
intervals. In this setting, drugs that prolong the refractory
period of the bypass tract should be used, especially those
that also block the AV node (by prolonging refractoriness).
Examples of such drugs include procainamide (class IA agent)
and propranolol (class II beta-blocker).
If wide-complex tachycardia is present and
the diagnosis of ventricular tachycardia cannot be excluded,
the drugs of choice are intravenous procainamide or amiodarone
(in lieu of cardioversion if the patient is stable hemodynamically).
Ibutilide may also be useful in this setting, although data
are lacking.
Importantly, avoid lidocaine in this setting.
It does not prolong refractoriness in the accessory pathway.
Lidocaine may increase the ventricular response if atrial fibrillation
is present.
Hemodynamically unstable tachycardia and
electrical cardioversion
In patients with a very fast ventricular
rate, hemodynamic instability (eg, hypotension, mental status
change) may ensue.
The initial treatment of choice in such patients
is direct-current synchronized electrical cardioversion.
Electrical cardioversion appears to terminate
most effectively the tachycardias due to reentry, such as AVNRT
and reciprocating tachycardias associated with WPW syndrome.
The electrical shock depolarizes all excitable
myocardium, lengthens refractoriness, interrupts reentrant circuits,
discharges foci, and establishes electrical homogeneity that
terminates reentry.
Because myocardial damage may occur with
increases in applied energy, the minimum effective energy should
be used and the energy should be titrated. An energy of at least
100 joules (monophasic or lower biphasic) successfully terminates
most SVTs and should be tried initially. If that fails, a second
shock with higher energy can be delivered.
Cardioversion can have several adverse effects.
It may induce arrhythmias because of inadequate synchronization,
with the shock occurring during the ST segment or T wave. Rarely,
even a properly synchronized shock can produce ventricular fibrillation.
Postcardioversion arrhythmias are generally transient and do
not require treatment. Embolic episodes may occur in 1-3% of
the patients converted from atrial fibrillation to sinus rhythm
if the episodes are longer than 48 hours.
Long-term maintenance treatment
Response to long-term antiarrhythmic therapy
for the prevention of further episodes of tachycardia in patients
with WPW syndrome remains quite variable and unpredictable.
Some drugs may paradoxically make the reciprocating tachycardia
more frequent. Dual-drug therapy has been used, eg, procainamide
and verapamil (class IA and IV), or quinidine and propranolol
(class IA and II). Good reasons exist to avoid quinidine and
procainamide; newer drugs that are safer and better are available.
Class IC drugs (eg, amiodarone, sotalol) are good choices, but
class IC drugs should not be given if the patient has structural
heart disease. Class IC drugs are typically used with an AV
nodal blocking agent.
The best plan is to not use drugs at all;
instead, refer all patients who have symptomatic WPW syndrome
for ablation because this cures the tachycardia and eliminates
the potential dangerous effects of drugs.
Patients who have accessory pathways with
short refractory periods are poor candidates for medical therapy
and are best treated with ablation.
Surgical Care: Ablative procedures are the
therapy of choice. Electrode catheters can be advanced intravenously
to locate and ablate the accessory tract by delivering electrical
or RF energy. Cryothermy, lasers, direct current, and microwave
energy sources have also been used in the past, but RF catheter
ablation has replaced these modalities because it is much more
efficacious, safe, and cost-effective.
RF ablation is currently the treatment of
choice for most adults and many children with symptomatic WPW
syndrome (ie, those who have AV reentrant tachycardia or atrial
flutter/fibrillation with conduction of the accessory pathway).
Success rates for catheter ablation exceed 90%.
Localization of the bypass tract(s)
First, perform an EP study to (1) determine
that the bypass tract is part of the tachycardia reentrant circuit,
and (2) locate the optimal site for ablation. Pathways can be
located in the left or right free wall or septum of the heart.
Multiple pathways may be present in approximately 5% of patients.
Pathways at all the sites in the heart and
in persons of all age groups can be ablated successfully. The
RF ablation creates conduction block that can be seen on intracardiac
electrogram findings (ie, during the EP study) between the atrial
activation and the bypass tract potential.
Identification of the ablation site during
EP studies
During the EP studies, direct recordings
of the accessory pathway indicate the optimal site for ablation.
The ventricular insertion site is indicated
by the earliest onset of the ventricular electrogram in relation
to the delta wave.
The atrial insertion site is indicated by
the region of the shortest VA interval during orthodromic tachycardia
(ie, AV reentrant tachycardia) or ventricular pacing.
Successful ablation sites show stable fluoroscopic
and electrical features. During orthodromic AV reentrant tachycardia,
the time between the ventricular and atrial potentials is short
and a pathway potential may be observed.
Generally, a thermistor-tipped catheter is
used, which shows a stable rise in catheter tip temperature,
suggesting catheter stability and optimal catheter-tissue contact.
The tip temperature generally rises above 50°C.
Indications for RF ablation
Patients with symptomatic AV reentrant tachycardia
should receive RF ablation.
Atrial fibrillation or other atrial tachyarrhythmias
that have rapid ventricular response via a bypass tract is an
indication for RF ablation procedures.
Patients with AV reentrant tachycardia or
atrial fibrillation with rapid ventricular rates found incidentally
during EP studies for unrelated arrhythmia should undergo RF
ablation.
Asymptomatic patients with ventricular preexcitation
whose livelihood, profession, insurability, or mental well-being
may be influenced by unpredictable tachyarrhythmias or in whom
such tachyarrhythmias would endanger the public safety should
have an RF ablation procedure.
Patients with atrial fibrillation and a controlled
ventricular response via the bypass tract are candidates for
RF ablation.
Patients with a family history of sudden
cardiac death should undergo RF ablation.
Effectiveness of RF ablation: A survey by
the North American Society for Pacing and Electrophysiology
(NASPE) indicates that ablation is successful. Results are as
follows:
For left free wall accessory pathways, 2312
of 2527 patients (91%) were cured.
For septal accessory pathways, 1115 of 1279
patients (87%) were cured.
For right free wall accessory pathways, 585
of 715 patients (82%) were cured.
Complications of RF ablation
In the United States, complications have
been reported in 94 of 4521 patients (2.1%). Of the 4521 patients,
13 died (0.2%).
In Europe, the complication rate is reported
to be 4.4%. Of 2222 patients, 3 died.
Surgical ablation
Surgical open heart procedures were more
common before RF ablation was developed.
Now, RF catheter ablation has virtually eliminated
surgical open heart treatments in the vast majority of patients,
with the following exceptions:
Patients in whom RF catheter ablation (with
repeated attempts) fails
Patients undergoing concomitant cardiac surgery
(possible exception)
Patients with other tachycardias with multiple
foci who require surgical intervention (very rare)
Consultations: Specific subspecialty consultations
are often needed. These may include any of the following:
Cardiovascular specialist
Electrophysiologist
Pediatric cardiovascular specialist
Diet:
The majority of patients presenting with
WPW syndrome are not elderly.
Patients presenting with structural heart
disease, cardiomyopathy, or heart failure may require a low-salt,
low-cholesterol diet.
Activity: Generally, no activity restrictions
are recommended in patients with ECG findings of preexcitation
but without tachycardias. They should be restricted from high-risk
professions (eg, airline pilot) and may be restricted from competitive
sports.
Patients presenting with tachycardias and
accessory pathways should avoid participating in competitive
sports because catecholamines can decrease the refractoriness
of the bypass tract and facilitate tachyarrhythmias.
Patients with hypertrophic cardiomyopathy
or the Ebstein anomaly should also abstain from competitive
sports.
Once a curative procedure (eg, RF ablation
of the accessory pathway) has been successfully performed, most
patients can return to competitive sports several months later.
MEDICATION
The goals of pharmacotherapy are to reduce
morbidity and to prevent complications.
Drug Category: Antiarrhythmic agents -- Prolong
refractory period of the conduction tissue, the accessory pathway,
or both.
Drug Name
| Drug
Name |
Adenosine (Adenocard) -- Blocks conduction
time in the AV node. Can interrupt AVRT by blocking conduction
in the AV node to restore normal sinus rhythm in PSVT,
including PSVT associated with WPW syndrome. Should not
be given to patients with preexcitation. |
| Adult
Dose |
6 mg rapid IV bolus over 1-2 s initially;
if no response within 1-2 min, give 12 mg rapid IV bolus;
repeat 12-mg dose second time prn; not to exceed doses
>12 mg |
| Pediatric
Dose |
0.1 mg/kg IV; repeat at 0.2
mg/kg if first dose not effective; not to exceed 12 mg
Alternatively, 0.05 mg/kg IV; if not effective within
2 min, increase dose by 0.05-mg/kg increments q2min; not
to exceed 0.25 mg/kg
|
| Contraindications |
Documented hypersensitivity; second- or
third-degree AV block or sick sinus syndrome (except in
patients with functioning artificial pacemaker); atrial
flutter; atrial fibrillation; ventricular tachycardia |
| Interactions |
Coadministration with carbamazepine may
produce higher degrees of heart block; dipyridamole may
potentiate effects; methylxanthines may antagonize effects;
do not administer to patients with a heart transplant |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Adenosine-induced bronchoconstriction
possible in patients with asthma
May cause prolonged asystole in patients with a heart
transplant; may provoke atrial fibrillation
|
| Drug
Name |
Propranolol (Inderal) -- Class II antiarrhythmic
nonselective beta-adrenergic receptor blocker with membrane-stabilizing
activity that decreases automaticity of contractions. |
| Adult
Dose |
1-3 mg IV under careful monitoring; not
to exceed 1 mg/min to avoid lowering blood pressure and
causing cardiac standstill; allow time for drug to reach
site of action |
| |
(particularly if slow circulation); administer
second dose after 2 min prn thereafter, not to be administered
sooner than 4 h after initial dose; do not continue doses
after desired alteration in rate or rhythm achieved; switch
to PO as soon as clinically indicated; 10-30 mg tid/qid
(usual) |
| Pediatric
Dose |
2-4 mg/kg/d PO divided bid (ie, 1-2 mg/kg
bid); IV use not recommended; however, for arrhythmias,
dose of 0.01-0.1 mg/kg by slow push has been recommended;
not to exceed 1 mg/dose; change to PO as soon as clinically
indicated |
| Contraindications |
Documented hypersensitivity; uncompensated
CHF; bradycardia; cardiogenic shock; AV conduction abnormalities |
| Interactions |
Coadministration with aluminum salts, barbiturates,
NSAIDs, penicillins, calcium salts, cholestyramine, and
rifampin may decrease effects; calcium channel blockers,
cimetidine, loop diuretics, and MAOIs may increase toxicity;
toxicity of hydralazine, haloperidol, benzodiazepines,
and phenothiazines may increase |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Beta-adrenergic blockade may decrease signs
of acute hypoglycemia and hyperthyroidism; abrupt withdrawal
may exacerbate symptoms of hyperthyroidism, including
thyroid storm; withdraw drug slowly and monitor closely |
| Drug
Name |
Verapamil (Verelan, Calan) -- By interrupting
reentry at AV node, can restore normal sinus rhythm in
patients with PSVT |
| Adult
Dose |
80-160 mg PO tid; alternatively, 5-10 mg
IV followed by second dose 15-30 min later if patient
does not respond satisfactorily to initial dose; extended-release
dosage form may be given qd |
| Pediatric
Dose |
Not established |
| Contraindications |
Documented hypersensitivity; severe CHF;
sick sinus syndrome or second- or third-degree AV block;
hypotension (<90 mm Hg systolic) |
| Interactions |
May increase carbamazepine, digoxin, and
cyclosporine levels; coadministration with amiodarone
can cause bradycardia and a decrease in cardiac output;
when administered concurrently with beta-blockers, may
increase cardiac depression; cimetidine may increase levels;
may increase theophylline levels |
| Pregnancy |
B - Usually safe but benefits must outweigh
the risks. |
| Precautions |
Hepatocellular injury may occur; transient
elevations of transaminases with and without concomitant
elevations in alkaline phosphatase and bilirubin have
occurred (elevations have been transient and may disappear
with continued treatment); monitor liver function periodically |
| Drug
Name |
Digoxin (Lanoxin) -- Has direct inotropic
effects in addition to indirect effects on the cardiovascular
system. However, may shorten refractory period. Most deaths
in WPW have been associated with digoxin use. |
| Adult
Dose |
NOT RECOMMENDED; has been associated with
ventricular fibrillation |
| Pediatric
Dose |
5-10 years: 20-35 mcg/kg PO
>10 years: 10-15 mcg/kg PO
Maintenance dose: 25-35% of PO loading dose
|
| Contraindications |
Documented hypersensitivity; ADULT PATIENTS;
beriberi heart disease, idiopathic hypertrophic subaortic
stenosis, constrictive pericarditis, and carotid sinus
syndrome |
| Interactions |
IV calcium may produce arrhythmias in digitalized
patients; medications that may increase levels include
alprazolam, benzodiazepines, bepridil, captopril, cyclosporine,
propafenone, propantheline, quinidine, diltiazem, aminoglycosides,
oral amiodarone, anticholinergics, diphenoxylate, erythromycin,
felodipine, flecainide, hydroxychloroquine, itraconazole,
nifedipine, omeprazole, quinine, ibuprofen, indomethacin,
esmolol, tetracycline, tolbutamide, and verapamil
Medications that may decrease serum levels include aminoglutethimide,
antihistamines, cholestyramine, neomycin, penicillamine,
aminoglycosides, oral colestipol, hydantoins, hypoglycemic
agents, antineoplastic treatment combinations (including
carmustine, bleomycin, methotrexate, cytarabine, doxorubicin,
cyclophosphamide, vincristine, procarbazine), aluminum
or magnesium antacids, rifampin, sucralfate, sulfasalazine,
barbiturates, kaolin/pectin, and aminosalicylic acid
|
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Hypokalemia may reduce positive inotropic
effect of digitalis; hypercalcemia predisposes patient
to digitalis toxicity, and hypocalcemia can make digoxin
ineffective until serum calcium levels are normal; magnesium
replacement therapy must be instituted in patients with
hypomagnesemia to prevent digitalis toxicity; patients
diagnosed with incomplete AV block may progress to complete
block when treated with digoxin; exercise caution in hypothyroidism,
hypoxia, and acute myocarditis; adjust dose in renal impairment;
highly toxic (overdoses can be fatal) |
| Drug
Name |
Procainamide (Procanbid, Pronestyl) -- Class
IA antiarrhythmic. Increases refractory period of atria,
ventricles, and accessory pathway. Excellent in preexcited
atrial fibrillation or flutter. |
| Adult
Dose |
30 mg/min IV continuous infusion until arrhythmia
suppressed, patient becomes hypotensive, QRS widens 50%
above baseline, or maximum dose of 17 mg/kg administered;
once arrhythmia suppressed, may infuse at continuous rate
of 1-4 mg/min |
| Pediatric
Dose |
Not established; suggested
as follows:
15-50 mg/kg/d PO divided q3-6h; not to exceed 4 g/d
20-30 mg/kg/d IM divided q4-6h; not to exceed 4 g/d
3-6 mg/kg/dose IV infused over 5 min
Maintenance dose: 20-80 mcg/kg/min administered as continuous
infusion; not to exceed 100 mg/dose or 2 g/d
|
| Contraindications |
Documented hypersensitivity; torsade de
pointes; systemic lupus erythematosus |
| Interactions |
Can expect increased levels of procainamide
metabolite NAPA in patients taking cimetidine, ranitidine,
beta-blockers, amiodarone, trimethoprim, and quinidine;
may increase effect of skeletal muscle relaxants, quinidine
and lidocaine, and neuromuscular blockers; ofloxacin inhibits
tubular secretion of procainamide and may increase bioavailability;
when taken concurrently with sparfloxacin, may increase
risk of cardiotoxicity |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Monitor for hypotension; plasma concentrations
and active metabolite (NAPA) may increase in renal failure;
high or toxic concentrations may induce AV block or abnormal
automaticity; toxicity may outweigh benefit long term;
do not use as a first-line drug for WPW syndrome |
| Drug
Name |
Quinidine (Quinaglute, Quinidex, Cardioquin)
-- Maintains normal heart rhythm and converts atrial fibrillation
or flutter. Not recommended as first-line drug for WPW
syndrome. |
| Adult
Dose |
200 mg PO q2-3h for 5-8 doses with subsequent
daily increases until sinus rhythm restored or adverse
effects occur; not to exceed 3-4 g/d |
| Pediatric
Dose |
30 mg/kg/d PO in 5 divided doses |
| Contraindications |
Documented hypersensitivity; complete AV
block or intraventricular conduction defects; presently
taking ritonavir or sparfloxacin |
| Interactions |
Phenytoin, rifampin, and phenobarbital may
decrease concentrations; toxicity increased when taken
with ritonavir, sparfloxacin, beta-blockers, amiodarone,
verapamil, cimetidine, alkalinizing agents, or nondepolarizing
or depolarizing muscle relaxants; may enhance effect of
anticoagulants |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Caution in G-6-PD deficiency and those with
tendency to develop granulocytopenia; avoid use in myocardial
depression, hepatic or renal insufficiency, and myasthenia
gravis |
| Drug
Name |
Amiodarone (Cordarone, Pacerone) -- May
inhibit AV conduction and sinus node function. Prolongs
action potential and refractory period in myocardium and
inhibits adrenergic stimulation. |
| Adult
Dose |
Loading dose: 800-1600 mg/d
PO in 1-2 doses for 1-3 wk; decrease to 600-800 mg/d in
1-2 doses for 1 mo
Maintenance dose: 400 mg/d PO; alternatively, 150 mg (10
mL) IV over first 10 min, followed by 360 mg (200 mL)
over next 6 h, then 540 mg over next 18 h
|
| Pediatric
Dose |
10-15 mg/kg/d or 600-800 mg/1.73 m2/d PO
for 4-14 d or until adequate control of arrhythmia attained |
| Contraindications |
Documented hypersensitivity; complete AV
block; intraventricular conduction defects; taking ritonavir
or sparfloxacin |
| Interactions |
Increases effect and blood levels of theophylline,
quinidine, procainamide, phenytoin, methotrexate, flecainide,
digoxin, cyclosporine, beta-blockers, and anticoagulants;
cardiotoxicity increased by ritonavir, sparfloxacin, and
disopyramide; coadministration with calcium channel blockers
may cause additive effect and further decrease myocardial
contractility; cimetidine may increase level |
| Pregnancy |
C - Safety for use during pregnancy
has not been established. |
| Precautions |
Caution in thyroid or liver disease |
| Drug
Name |
Sotalol (Betapace) -- Class III antiarrhythmic
agent that blocks potassium channels, prolongs action
potential duration, and lengthens QT interval. Noncardiac
selective beta-adrenergic blocker. |
| Adult
Dose |
80 mg PO bid; increase dose gradually q2-3d
to 240-320 mg/d |
| Pediatric
Dose |
Not established |
| Contraindications |
Documented hypersensitivity; long QT, history
of torsades de pointes |
| Interactions |
Aluminum salts, barbiturates, NSAIDs, penicillins,
calcium salts, cholestyramine, and rifampin may decrease
bioavailability and plasma levels, possibly resulting
in decreased pharmacologic effect; cardiotoxicity may
increase when administered concurrently with sparfloxacin,
calcium channel blockers, quinidine, flecainide, and contraceptives;
toxicity increases when administered concurrently with
digoxin, flecainide, acetaminophen, clonidine, epinephrine,
nifedipine, prazosin, haloperidol, phenothiazines, and
catecholamine-depleting agents |
| Pregnancy |
B - Usually safe but benefits must outweigh
the risks. |
| Precautions |
Beta-adrenergic blockade may decrease signs
and symptoms of acute hypoglycemia and clinical signs
of hyperthyroidism; abrupt withdrawal may exacerbate symptoms
of hyperthyroidism, including thyroid storm; withdraw
drug slowly and monitor patient closely; caution in hypokalemia,
peripheral vascular disease, hypomagnesemia, and CHF |
| Drug
Name |
Diltiazem (Cardizem, Dilacor, Tiamate, Tiazac)
-- Slows AV nodal conduction. |
| Adult
Dose |
IR: 30-90 mg PO q8h
SR: 120-300 mg PO qd
IV: 10-20 mg bolus over 10-20 min, followed by continuous
infusion at 10-15 mg/h
|
| Pediatric
Dose |
Not established |
| Contraindications |
Documented hypersensitivity;
severe CHF; sick sinus syndrome; second- or third-degree
AV block; hypotension (<90 mm Hg systolic) |
| Interactions |
May increase carbamazepine, digoxin, cyclosporine,
and theophylline levels; when administered with amiodarone,
may cause bradycardia and decrease in cardiac output;
when given with beta-blockers, may increase cardiac depression;
cimetidine may increase levels |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Caution in impaired renal or hepatic function;
may increase LFT levels, and hepatic injury may occur |
| Drug
Name |
Ibutilide (Corvert) -- Class III antiarrhythmic
agent that may work by increasing action potential duration,
thereby changing atrial cycle length variability. Mean
time to conversion is 30 min. Two thirds of patients who
converted were in sinus rhythm at 24 h. Ventricular arrhythmias
occurred in 9.6% of patients and were mostly PVCs. The
incidence of torsades de pointes was <2%. |
| Adult
Dose |
<60 kg: 0.01 mg/kg IV over 10 min
>60 kg: 1 mg IV over 10 min
|
| Pediatric
Dose |
Not established |
| Contraindications |
Documented hypersensitivity |
| Interactions |
Increases toxicity of quinidine and procainamide;
concurrent administration with TCAs and phenothiazines
may prolong QT interval; toxicity of digoxin increases
when administered concurrently |
| Pregnancy |
C - Safety for use during pregnancy has
not been established |
| Precautions |
Caution in renal or hepatic impairment |
| Drug
Name |
Dofetilide (Tykosin) -- Increases
monophasic action potential duration, primarily due to
delayed repolarization. Terminates induced reentrant tachyarrhythmias
(eg, atrial fibrillation/flutter, ventricular tachycardia)
and prevents their reinduction. No data in WPW syndrome. |
| Adult
Dose |
125-500 mcg IV bid; must be started in an
inpatient monitored setting |
| Pediatric
Dose |
Not established |
| Contraindications |
Documented hypersensitivity; concomitant
use of verapamil or the cation transport system inhibitor
cimetidine, trimethoprim (alone or in combination with
sulfamethoxazole), or ketoconazole; congenital or acquired
long QT syndromes; severe renal impairment (CrCl <20
mL/min); prochlorperazine and megestrol coadministration;
a baseline QT interval or QTc >440 ms (500 ms in patients
with ventricular conduction abnormalities) |
| Interactions |
Verapamil, TMP/SMZ, ketoconazole, potassium-depleting
diuretics, digoxin, cimetidine, phenothiazines, triamterene,
metformin, prochlorperazine, amiloride, megestrol, and
antiarrhythmic agents may increase toxicity |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Maintain potassium levels within reference
range prior to and during administration; to minimize
risk of induced arrhythmia, calculations of CrCl and continuous
ECG monitoring required; cardiac resuscitation equipment
and personnel must be present |
| Drug
Name |
Flecainide (Tambocor) -- Blocks sodium channels,
producing dose-related decrease in intracardiac conduction
in all parts of heart. Increases electrical stimulation
of threshold of ventricle, His-Purkinje system. Shortens
phase 2 and phase 3 repolarization, resulting in decreased
action potential duration and ERP.
Indicated for the treatment of paroxysmal atrial fibrillation/flutter
associated with disabling symptoms and PSVT, including
AVNRT, AV reentrant tachycardia, and other SVTs of unspecified
mechanism associated with disabling symptoms in patients
without structural heart disease. Also indicated for prevention
of documented life-threatening ventricular arrhythmias,
such as sustained ventricular tachycardia.
Not recommended in less severe ventricular arrhythmias,
even if patients are symptomatic.
|
| Adult
Dose |
100 mg PO bid q12h; increase q4d but not
to exceed 400 mg/d |
| Pediatric
Dose |
3-6 mg/kg/d or 100-150 mg/m2/d divided tid
to 11 mg/kg/d or 200 mg/m2/d |
| Contraindications |
Documented hypersensitivity; preexisting
second- or third-degree AV block, RBBB associated with
left hemiblock (bifascicular block) or trifascicular block,
unless a pacemaker is present to sustain cardiac rhythm
if complete heart block occurs; concurrent use of ritonavir
or amprenavir; recent MI |
| Interactions |
May increase toxicity of digoxin; beta-adrenergic
blockers, verapamil, and disopyramide may have additive
inotropic effects when administered with flecainide; CYP4502D6
inhibitors (eg, ritonavir, cimetidine, amiodarone) may
increase serum levels and cardiotoxicity |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Caution in preexisting sinus node dysfunction,
history of CHF, sick sinus syndrome, post MI, or myocardial
dysfunction; reserve use for life-threatening arrhythmias
only because deaths have been associated with proarrhythmic
effects of class IC antiarrhythmics; typically used in
conjunction with an AV nodal blocking agent; adjust dose
in renal or hepatic impairment |
| Drug
Name |
Propafenone (Rythmol) -- Shortens upstroke
velocity (phase 0) of monophasic action potential. Reduces
fast inward current carried by sodium ions in Purkinje
fibers and, to a lesser extent, myocardial fibers. May
increase diastolic excitability threshold and prolong
ERP. Reduces spontaneous automaticity and depresses triggered
activity. Indicated for treatment of documented life-threatening
ventricular arrhythmias, such as sustained ventricular
tachycardia. Appears to be effective in the treatment
of SVTs, including atrial fibrillation and flutter. Not
recommended in patients with less severe ventricular arrhythmias,
even if patients are symptomatic. |
| Adult
Dose |
150 mg PO q8h; increase at 3- to 4-d intervals,
not to exceed 300 mg q8h |
| Pediatric
Dose |
Not established |
| Contraindications |
Documented hypersensitivity, second- or
third-degree AV block, RBBB associated with left hemiblock
(bifascicular block) or trifascicular block; concurrent
use of ritonavir or amprenavir |
| Interactions |
Rifampin may decrease plasma levels; quinidine
may increase pharmacologic effects; may increase plasma
levels of beta-blockers, cyclosporine, warfarin, and digoxin;
CYP4502D6 inhibitors (eg, ritonavir, cimetidine, amiodarone)
may increase serum levels and cardiotoxicity |
| Pregnancy |
C - Safety for use during pregnancy has
not been established. |
| Precautions |
Caution in preexisting sinus node dysfunction,
history of CHF, sick sinus syndrome, post MI, or myocardial
dysfunction; reserve use for life-threatening arrhythmias
only because deaths have been associated with proarrhythmic
effects of class IC antiarrhythmics; adjust dose in renal
or hepatic impairment; typically used in conjunction with
an AV nodal blocking agent |
FOLLOW-UP
Further Inpatient Care:
Patients with WPW syndrome who are admitted
to the hospital after initiation of medical treatment in the
emergency department may require further evaluation and management
as follows:
Continuous telemetry monitoring to look for
resurgence of tachyarrhythmia and the degree of control of the
ventricular rate in those with atrial fibrillation
Initiation, dose adjustment, and maintenance
of long-term antiarrhythmic drugs for preventing recurrences
(However, patients generally undergo ablation.)
Laboratory evaluation and correction of electrolyte
and metabolic abnormalities that may have acted as triggers
Evaluation for associated underlying structural
cardiac defects, such as Ebstein anomaly and hypertrophic cardiomyopathy,
is as follows:
EP evaluation of patients who meet the indications,
including the following:
To diagnose and locate accessory pathways
and the reentrant pathways or sites of origin of SVTs
To define appropriate therapy
To test the results of therapy
To enable electrocardiographically guided
therapy such as RF ablation
RF ablation for patients who are candidates
for such therapy, including the following:
Patients with symptomatic tachycardia who
cannot tolerate drug therapy or whose conditions are resistant
to such therapy
Patients who have atrial fibrillation with
a rapid ventricular response via a bypass tract who cannot tolerate
drug therapy or whose conditions are resistant to such therapy
Patients who have AV reentrant tachycardia
or atrial fibrillation with rapid ventricular rates found during
EP studies
Asymptomatic patients whose profession, insurability,
mental well-being, or responsibility to public safety may be
affected by unpredictable occurrence of tachyarrhythmias
Patients with a family history of sudden
cardiac death
Monitor drug use.
Carefully monitor for proarrhythmias, especially
when procainamide, quinidine, amiodarone, or sotalol are initiated.
A few days of inpatient telemetry monitoring, including determination
of QT interval lengthening on ECG readings, is required for
these agents. An increase in the QT interval of 25% or greater
should be avoided.
Surgical ablation is recommended in certain
patients, including the following:
Patients in whom RF catheter ablation fails
Patients who will be undergoing concomitant
cardiac surgery
Patients with atrial tachycardias who have
multiple foci (sometimes)
Further Outpatient Care:
Patients need to continue antiarrhythmic
therapy as prescribed. If symptoms related to tachyarrhythmias
recur, patients should inform the physician.
Arrange follow-up visits to assess for the
recurrence of arrhythmia, the effectiveness of antiarrhythmic
therapy, and adverse effects of medications.
Follow-up ECG or Holter monitoring may be
needed to assess for changes in QT duration and the recurrence
of arrhythmias or proarrhythmias.
Patients who take amiodarone require careful
periodic monitoring for adverse effects and organ toxicity,
including thyroid function tests, ophthalmic examination, pulmonary
function tests, and hepatic function tests.
Patients who undergo EP studies, RF ablation,
or surgical ablation may require monitoring of wound care following
hospital discharge. Further follow-up care to assess for the
recurrence of arrhythmia is also needed.
Patients with underlying structural heart
disease, such as the Ebstein anomaly, may require follow-up
care by a specialist pediatric cardiologist.
If a patient with WPW syndrome dies suddenly,
siblings and first-degree relatives should be screened for preexcitation.
Unless curative ablation has been performed,
patients should refrain from participating in competitive sports.
Routine EP studies are not recommended following
RF ablation solely to ensure that the ablation was curative,
unless patients become symptomatic.
Asymptomatic patients with only the ECG findings
of preexcitation should be seen at frequent intervals and should
not undergo any aggressive EP evaluation or pharmacologic or
ablative therapy unless they become symptomatic or their profession,
insurability, mental well-being, or the safety of the public
may be affected by unpredictable occurrence of tachyarrhythmias.
In/Out Patient Meds:
Adenosine
Digoxin (not recommended for WPW syndrome
in adults)
Propranolol
Verapamil
Quinidine
Procainamide
Amiodarone
Sotalol
Transfer:
Certain patients with WPW syndrome must be
transferred to a tertiary facility for comprehensive evaluation
and management by a cardiac electrophysiologist, which may include
EP studies or ablative therapy. Such patients include those
presenting with any of the following:
Sudden death
Syncope
Significant symptomatic tachyarrhythmias
Uncertain diagnosis in those with wide-complex
tachycardia
Associated structural heart disease, eg,
Ebstein anomaly, cardiomyopathy, mitral valve prolapse.
WPW syndrome who have a family history of
sudden death
Asymptomatic but with WPW syndrome who are
in professions in which spontaneous occurrence of tachyarrhythmia
may jeopardize public safety, cause much mental anguish, or
influence insurability
Atrial fibrillation or flutter
Deterrence/Prevention:
WPW syndrome is largely congenital or hereditary.
No particular method exists to eliminate the possibility of
developing accessory pathways. In the future, genetic recognition
and counseling may become a useful tool.
Fortunately, the majority of patients with
ECG findings of preexcitation do not develop tachyarrhythmias.
Patients who present with tachyarrhythmic
symptoms require drug therapy to prevent further episodes. Such
long-term therapy may include the use of amiodarone, sotalol,
quinidine and propranolol, and verapamil and diltiazem on a
regular basis.
If the procedure is successful, patients
who have undergone ablative treatment are usually cured of the
disease and are not at risk for further tachyarrhythmias.
Complications:
Tachyarrhythmia
Palpitations
Dizziness or syncope
Sudden cardiac death
Complications of drug therapy (eg, proarrhythmia,
organ toxicity)
Complications associated with invasive procedures
and surgery
Recurrence
Prognosis:
Patients with only preexcitation on their
ECG findings who are asymptomatic generally have a very good
prognosis. Most of these patients do not develop symptoms in
their lifetime.
Patients with a family history of sudden
cardiac death or significant symptoms of tachyarrhythmias or
cardiac arrest have worse prognoses. However, once definitive
therapy is performed, including curative ablation, the prognosis
is once again excellent.
Asymptomatic patients should not be evaluated
by EP testing unless they are in a high-risk profession. Risk
stratification is not generally needed for asymptomatic patients.
Patient Education:
Patient education is of paramount importance
in patients with WPW syndrome. This is especially true in asymptomatic
young patients who have been told of their abnormal ECG results.
Reassurance and periodic follow-up care of such patients is
necessary.
Educate patients who are being treated with
drug therapy thoroughly regarding the disease and the type of
medications they are taking. Such patients must be taught the
following:
How to recognize disease recurrence
How to perform vagal maneuvers, when needed
To keep their follow-up appointments
To identify the adverse effects of antiarrhythmic
drugs
To avoid competitive sports
To learn about ablative options and the indications
for ablation, should they become candidates in future
Patients with WPW syndrome should also educate
their family members, and their siblings should be screened
for preexcitation.
MISCELLANEOUS
Medical/Legal Pitfalls:
Evaluate patients presenting with symptomatic
tachycardia (SVT or wide-complex tachycardia) for the presence
of preexcitation on the ECG results.
Evaluate patients with WPW syndrome for the
presence of very short refractory periods because these patients
carry higher probabilities of developing symptoms or complications.
Such patients also respond poorly to drug therapy. Identify
these patients, even if asymptomatic, and treat them aggressively
using EP evaluations and ablative therapy.
Special Concerns:
Children with symptomatic WPW syndrome who
undergo RF ablation sustain myocardial damage or injury. How
this damaged myocardium will change as children grow is still
not known.
Evaluate patients with Ebstein anomaly for
multiple accessory pathways. During EP studies and ablation,
all such pathways should be recognized and treated.